
A unique transportation system was designed at the Heathrow airport called the Heathrow pod. It is a carbon-free transport option (engineered by Ultra Global PRT) that is dedicated for connecting Terminal 5 to the business car park that is located in the north side of the airport. These pods are electric and autonomous with user-friendly touchscreens for the riders to choose their destination. The wait time for the pod is only around 10 seconds, and that is if the pod is not available at the instance the user reaches the station. Transportation via these pods made an excellent substitute to the traditional bus journeys that would account for about 70,000 trips and 100 ton of carbon dioxide emission. The pods can carry around 2,500 riders per hour per direction, which is the same capacity that cable cars have; only that the pods cost half as much and are going to continue to decrease. They travel at 25 mph on a 1.5-meter track, weigh around 800 kg, carry 4 passengers, and operate with 7 kW AC motors powered by 45 Ah lead batteries. Average energy usage per rider is 0.59 MJ per kilometre, which makes it 70% more efficient than a car. The route is set up by the pod’s central control system and it safely sticks to the route by identifying their lateral/longitudinal position with ultrasonic and laser sensors. The pods are constructed to be aerodynamic to neglect wind effects and obstacles such as ice or rocks are removed with additional devices that are in part with the pathways. This information was obtained from theengineer.co.uk. The development of the pods encouraged other companies such as Westfield Sportscars and Oxbotica to create their own fully autonomous pods also.
The Heathrow pods are a type of Personal Rapid Transit systems (PRTs) and it is important that these vehicles are efficient. Lees-Miller2 discusses about minimising waiting time for passengers in PRTs. He proposes mathematical models regarding congestion on the track, congestion in stations, and the availability and whereabouts of empty vehicles. This study neglects the congestion time on the track and in stations but most PRTs including the Heathrow pods do not suffer from such issues anyway, therefore it is a safe assumption.
Figure 1 shows the mathematical formula describing the condition. The notations for subscripts and variables as well as definitions are stated in Reference 2, therefore the reader should consider checking it if further elaboration is desired.
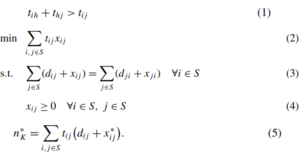
Figure 1 – Trip time matrix, objective function, constants, boundary conditions, and optimal solution2, respectively.
Equation 1 claims that if there is a time penalty at a station h in between station i and j, then the quickest time taken from station i to j is delayed. Equation 2 is the number of vehicles that are required to sustain the flows of empty vehicles in average. Equation 3 shows flow conservation constraints that makes sure the total number of vehicles remains constant. Equation 4 is a boundary condition in the system. Equation 5 defines the minimum number of vehicles required to serve the rides. Incorporating three different methods, M/G/s queuing model, SNN, and MDP model with these mathematical formulae, the M/G/s model showed complementary average waiting times to those obtained by the SNN heuristic. MDP showed longer average waiting times, especially when the fleet size was small. As the fleet size increased, the productivity increased.
One of the major missions that the city of London is aiming to establish lies in the healthcare industry. The plan is to benefit all Londoners from digital health and social care by connecting NHS data with other initiatives through MedTech programme. An accelerator firm, DigitalHealth is supporting the programme by scaling medical products and services. ‘Innovation Surgeries’ are one example that provide networking opportunities and support in accessing the NHS. This can come with a combination of robotic surgical procedures to make up for the understaffed situation and innovative data usage dedicated to increase the performance level across public services. For instance, a patient’s data is shared with the NHS server, thereby prioritising the patients accordingly to the severity. Doctors would not have to diagnose patients as thoroughly and nurses would pre-acquire their information, which would significantly increase the productivity.
There are many types of robotic surgeries such as for tumours, spine, or lung cancer. One common trait robotic surgeries share is that they aim to be minimally invasive. The procedure may vary freely, depending on the surgery type, from a remote-controlled endoscope to a telemanipulator. A well-known example of a surgical telemanipulator is the da Vinci system. The da Vinci system is composed of multiple ergonomic robotic arms that are controlled by the surgeon. The structure is based on a master-slave system with functional units of operator console, vision cart, and patient cart.
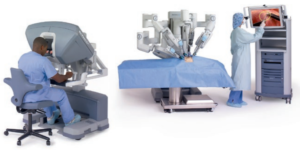
Figure 2 – Operator console (master), vision cart (control), and patient card (slave), respectively from the leftside3
Figure 2 shows how it looks during a procedure. It interacts with its surroundings such as the operator, nurses, audio systems, screen display, and other crucial factors in a surgical room. An essential component for robotic or – telesurgery is the data transmission speed from the controller to the system. Network latency affects surgical performance exponentially; a short delay of 250 milliseconds dramatically increases the surgery duration compared to a traditional surgery4. The latency lag may also make the procedure feel less natural, which might lower the quality of surgery. Telesurgery allows doctors to operate from a different place to where the patient is located, but fibreoptic network may be required if the distance is too far. Simply put, telesurgery is a combination of image calibration, sensors, and mechatronic kinematics. If the latency lag does not exist, it is arguably better as it completely eliminates hand tremor. The system projects the image of the surgical site atop the surgeon’s hands, restoring hand-eye coordination and providing a natural correspondence in motions6. Additionally, the controller transforms the spatial motion of the tools into the camera frame of reference, so that the surgeon feels as if his or her hands are inside the patient’s body6.
Figure 3 shows a principal system diagram of the control architecture. UI manages user inputs, CPT manages mathematical calculations in serve modes, and the kernel implements servo loop closure. The MSD (multiple servo drive) boards handles servo amplifiers and the health monitoring network records errors and manipulates amplifiers through FRL (fault reaction logic function). FRL deals with the system’s time to achieve a safe state when there is a “fail-high” logic. In-depth information can be sought from Reference 6.
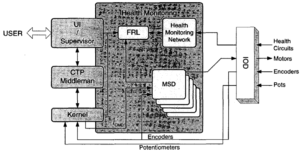
Figure 3 – Fundamental system architecture of da Vinci surgical system6
Civic Innovation Challenge is an initiative that collaborates with leading companies and organisations to face London’s social/environmental challenges. One of the challenges it faces is called Active Travel that intends to cut down unnecessary car journeys. Its milestone is to reach a bold 80% of trips being completed on foot, cycle, or public transportation by 2041. The current level is 63%, which makes the goal quite plausible. Stars Tfl came up with 2 potential solutions to contribute to the statistics: Park and Stride, and Car-free days. Park and Stride motivates parents to park their car a distance from school and walk the rest of the way5. This promotes physical activity, better air quality, and congestion-free roads near schools that improves safety. Car-free days encourage parents and staff to walk, cycle, or use public transport to get to school. Schools can carry out a survey to identify how many people drive and inform the borough to select a date for the car-free day. This can be promoted through school newspapers.
Reference
1 Trust for London. (2019). London’s population over time. [online] Available at: https://www.trustforlondon.org.uk/data/londons-population-over-time/ [Accessed 18 Sep. 2019].
2 Lees-Miller, J. (2013). Minimising average passenger waiting time in personal rapid transit systems. Annals of Operations Research, 236(2), pp.405-424.
3 Douissard, J., Hagen, M. and Morel, P. (2019). The da Vinci Surgical System. Bariatric Robotic Surgery, pp.13-27.
4 Diana, M. and Marescaux, J. (2015). Robotic surgery. British Journal of Surgery, 102(2), pp.e15-e28.
5 Stars.tfl.gov.uk. (2019). Activities. [online] Available at: https://stars.tfl.gov.uk/Explore/Idea [Accessed 19 Sep. 2019].
6 Guthart, G. and Salisbury, J. (n.d.). The Intuitive/sup TM/ telesurgery system: overview and application. Proceedings 2000 ICRA. Millennium Conference. IEEE International Conference on Robotics and Automation. Symposia Proceedings (Cat. No.00CH37065).
Recent Comments